戦闘などのストレス下でのアドレナリン作用が、血管への作用で、血管内皮細胞の変化で脂質異常も糖尿リスクも挙がる、筋力はアップする。
文献:Webber BJ et al.Prevalence of and Risk Factors for Autopsy-Determined Atherosclerosis Among US Service Members, 2001-2011.JAMA. 2012;308(24):2577-2583.
戦闘または不慮の事故で死亡した米軍人3832人(男性98.3%)の検死解剖報告書を基に、米軍における現在のアテローム性動脈硬化症の有病率を推計。有病率は8.5%で、有病者は年齢が高かった。有病率の上昇と関連する心血管リスク因子は脂質異常症(年齢調整後の有病率比2.09)、高血圧(同1.88)、肥満(同1.47)だった。
Prevalence of and Risk Factors for Autopsy-Determined Atherosclerosis Among US Service Members, 2001-2011FREE
Bryant J. Webber, MD; Peter G. Seguin, MD, MPH; Daniel G. Burnett, MD, MPH; Leslie L. Clark, PhD, MS; Jean L. Otto, DrPH, MPH
[+-] Author Affiliations
Author Affiliations: Uniformed Services University of the Health Sciences, Bethesda, Maryland (Drs Webber and Burnett); Armed Forces Medical Examiner System, Dover Air Force Base, Delaware (Dr Seguin); Armed Forces Health Surveillance Center, Silver Spring, Maryland (Drs Clark and Otto); and Henry M. Jackson Foundation for the Advancement of Military Medicine Inc, Bethesda (Dr Otto).
JAMA. 2012;308(24):2577-2583. doi:10.1001/jama.2012.70830.
Text Size: AA A
Published online
Article
Tables
References
ABSTRACT
ABSTRACT | METHODS | RESULTS | COMMENT | AUTHOR INFORMATION | REFERENCES
Context Autopsies of US service members killed in the Korean and Vietnam wars demonstrated that atherosclerotic changes in the coronary arteries can appear early in the second and third decades of life, long before ischemic heart disease becomes clinically apparent.
Objective To estimate the current prevalence of coronary and aortic atherosclerosis in the US armed forces.
Design, Setting, and Participants Cross-sectional study of all US service members who died of combat or unintentional injuries in support of Operations Enduring Freedom and Iraqi Freedom/New Dawn between October 2001 and August 2011 and whose cardiovascular autopsy reports were available at the time of data collection in January 2012. Prevalence of atherosclerosis was analyzed by various demographic characteristics and medical history. Classifications of coronary atherosclerosis severity were determined prior to data analysis and designed to provide consistency with previous military studies: minimal (fatty streaking only), moderate (10%-49% luminal narrowing of ≥1 vessel), and severe (≥50% narrowing of ≥1 vessel).
Main Outcome Measures Prevalence of coronary and aortic atherosclerosis in the US armed forces and by age, sex, self-reported race/ethnicity, education, occupation, service branch and component, military rank, body mass index at military entrance, and International Classification of Diseases, Ninth Revision, Clinical Modification, diagnoses of cardiovascular risk factors.
Results Of the 3832 service members included in the analysis, the mean age was 25.9 years (range, 18-59 years) and 98.3% were male. The prevalence of any coronary atherosclerosis was 8.5% (95% CI, 7.6%-9.4%); severe coronary atherosclerosis was present in 2.3% (95% CI, 1.8%-2.7%), moderate in 4.7% (95% CI, 4.0%-5.3%), and minimal in 1.5% (95% CI, 1.1%-1.9%). Service members with atherosclerosis were significantly older (mean [SD] age, 30.5 [8.1] years) than those without (mean [SD] age, 25.3 [5.6] years; P < .001). Comparing atherosclerosis prevalence among with those with no cardiovascular risk factor diagnoses (11.1% [95% CI, 10.1%-12.1%]), there was a greater prevalence among those with a diagnosis of dyslipidemia (50.0% [95% CI, 30.3%-69.7%]; age-adjusted prevalence ratio [PR], 2.09 [95% CI, 1.43-3.06]), hypertension (43.6% [95% CI, 27.3%-59.9%]; age-adjusted PR, 1.88 [95% CI, 1.34-2.65]), or obesity (22.3% [95% CI, 15.9%-28.7%]; age-adjusted PR, 1.47 [95% CI, 1.10-1.96]), but smoking (14.1% [95% CI, 8.0%-20.2%]) was not significantly associated with a higher prevalence of atherosclerosis (age-adjusted PR, 1.12 [95% CI, 0.73-1.74]).
Conclusion Among deployed US service members who died of combat or unintentional injuries and received autopsies, the prevalence of atherosclerosis varied by age and cardiovascular risk factors.
Age-adjusted ischemic heart disease mortality rates in the United States have declined by 72% since their peak in 19681- 2—a phenomenon attributed about equally to reduction in risk factors and expansion of therapies.3- 4 These preventive and therapeutic advancements derive from an improved elucidation of the disease process. An early breakthrough in the understanding of the natural history of atherosclerotic heart disease was achieved in 1953, when Enos and colleagues5 at the Armed Forces Institute of Pathology reported a 77% prevalence of coronary atherosclerosis among US soldiers killed in the Korean War. By demonstrating anatomically that atherosclerosis affected a large proportion of young individuals without clinical evidence of heart disease, their study revolutionized the understanding of the onset and progression of cardiovascular disease.6 A follow-up report in the Vietnam War era,7 along with a number of autopsy studies in the civilian population,8- 14 provided additional evidence that the onset of atherosclerosis may occur at an early age.
Since the publication of these studies, health policies for children and young adults in the general population15- 16 as well as the military population17- 18 of the United States have been implemented to reduce the risk of cardiovascular disease associated with risk factors such as hypertension, diabetes, cholesterol, and smoking. We conducted a cross-sectional study to assess the current prevalence of autopsy-determined atherosclerosis among US service members who died in support of combat operations.
METHODS
ABSTRACT | METHODS | RESULTS | COMMENT | AUTHOR INFORMATION | REFERENCES
Every US service member who died in support of Operations Enduring Freedom (OEF) or Iraqi Freedom/New Dawn (OIF/OND) between October 2001 and August 2011 (OIF began in March 2003 and was renamed OND in September 2010) was included in this cross-sectional study. To maintain continuity with previous military studies, those with a manner of death labeled as “suicide,” “natural,” or “undetermined” were excluded. Active duty service members and activated reservists of all service branches (ie, Air Force, Army, Coast Guard, Marine Corps, and Navy) were eligible for entry. This study was approved by the Office of Research at the Uniformed Services University of the Health Sciences; as deceased persons research, it did not require institutional review board approval.
Autopsy, Demographic, and Diagnostic Data Sources
We obtained autopsy reports from the Armed Forces Medical Examiner Tracking System (AFMETS) and demographic and medical encounter data from the Defense Medical Surveillance System (DMSS). AFMETS, managed by the Mortality Surveillance Division of the Armed Forces Medical Examiner System, Dover, Delaware, is the central registry for US military fatalities.19 DMSS, managed by the Armed Forces Health Surveillance Center, Silver Spring, Maryland, is the central repository for medical surveillance data for the armed forces, which contains longitudinal data on service members, including almost complete ascertainment of all medical encounters since 1990, as well as demographic and deployment data.20
Demographic data included age, sex, race/ethnicity, highest education level achieved before death, occupation, service branch, active or reserve component, and military rank. On entering the military, service members self-select their race/ethnicity from a list of fixed categories; race/ethnicity was reported because of a known association with atherosclerosis.8- 9,13 Medical encounter data included body mass index (BMI, calculated as weight in kilograms divided by height in meters squared) at military entrance and history of atherosclerosis, ischemic heart disease, and major cardiovascular risk factors (ie, hypertension, dyslipidemia, obesity, diabetes mellitus, impaired fasting glucose, and smoking) based on International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM), codes. Service members were considered to have a history of any of these diseases or risk factors if they had at least 1 inpatient encounter or 2 outpatient encounters within 180 days with a defining diagnosis in any diagnostic position. All risk factor data were recorded prior to death.
Evaluation of Atherosclerotic Lesions
All US military deaths associated with combat or unintentional injuries in support of OEF or OIF/OND—whether the service member died in theater or after evacuation—required a comprehensive autopsy performed by a board-certified pathologist. For those who died in theater, autopsies were conducted at Dover Port Mortuary, Dover Air Force Base, Delaware, and were typically completed within 72 hours of death. For those who were wounded, medically evacuated, and subsequently died of wounds, autopsies were often conducted at the local military treatment facility, including National Naval Medical Center, Bethesda, Maryland (n = 32); Brooke Army Medical Center, Fort Sam Houston, Texas (n = 28); and Walter Reed Army Medical Center, Washington, DC (n = 20). Early in OEF, some autopsies were conducted at Landstuhl Regional Medical Center, Germany (n = 68).
All autopsies included an examination of the cardiovascular system. After removal of the heart from the pericardial sac and anterior chest chamber, the major coronary arteries (ie, left main, left anterior descending, circumflex, and right coronary) were inspected in the fresh state. The inferior portions of the ventricles were then sectioned and the valves opened according to the physiologic sequence of blood flow. The aorta was opened longitudinally, beginning typically at the aortic valve and carried distally through the bifurcation and into both common iliac arteries. The pathologist documented the location and degree of all atherosclerotic lesions based on gross examination.
To provide consistency with previous military studies, we determined the following classifications of coronary atherosclerosis severity prior to data analysis: minimal (fatty streaking only), moderate (10%-49% luminal narrowing of ≥1 vessel), and severe (≥50% narrowing of ≥1 vessel). We also documented the presence of aortic atherosclerosis.
Statistical Analyses
We used summary statistics to describe the population. We evaluated the prevalence of atherosclerosis by various demographic characteristics and diagnostic histories and reported unadjusted and Mantel-Haenszel age-adjusted prevalence ratios (PRs) with 95% confidence intervals. We used logistic regression to evaluate risk factor combinations and to assess for effect modification, reporting odds ratios (ORs). To compare included and excluded participants, we used χ2 and Fisher exact tests of homogeneity (for categorical variables) and unpaired t tests (for continuous variables).
All analyses were performed with Stata/IC version 11.2 (StataCorp). P values less than .05 were considered statistically significant; all P values were based on 2-sided tests.
RESULTS
ABSTRACT | METHODS | RESULTS | COMMENT | AUTHOR INFORMATION | REFERENCES
Of the 6191 fatalities in the case identification period, 4143 cases were identified by the Armed Forces Medical Examiner System (532 were initially excluded because the manner of death was other than combat or unintentional injury and 1516 because of injury to the cardiovascular system precluding complete autopsy). On review of the reports, we excluded an additional 311 cases (235 with no autopsy on file, 69 with damage preventing coronary examination, and 7 indicating organ donation). Included in the analysis were 3832 service members aged 18 to 59 years, of whom 98.3% were male.
Included and excluded participants were mostly homogenous demographically, although the excluded were younger (mean [SD] ages, 25.9 [6.2] vs 27.0 [6.6], respectively; P = .002) and had a smaller proportion of college graduates (10.0% vs 14.8%; P = .008); the groups had similar mean (SD) entrance BMIs (included, 24.3 [3.6] vs excluded, 24.4 [3.2]; P = .85) and similar proportions with 1 or more cardiovascular risk factor diagnoses (included, 8.5% vs excluded, 10.9%; P = .14).
Atherosclerosis Prevalence
The overall prevalence of coronary or aortic atherosclerosis was 12.1% (95% CI, 11.1%-13.1%). The prevalence of coronary and aortic atherosclerosis was 2.1% (95% CI, 1.7%-2.6%). The prevalence of any coronary atherosclerosis was 8.5% (95% CI, 7.6%-9.4%); severe coronary atherosclerosis was present in 2.3% (95% CI, 1.8%-2.7%), moderate in 4.7% (95% CI, 4.0%-5.3%), and minimal in 1.5% (95% CI, 1.1%-1.9%). The prevalence of any aortic atherosclerosis was 5.7% (95% CI, 5.0%-6.5%).
Factors Associated With Prevalent Atherosclerosis
Age consistently produced the strongest association with prevalent atherosclerosis. Service members with atherosclerosis (mean [SD] age, 30.5 [8.1] years) were approximately 5 years older than those without (mean [SD] age, 25.3 [5.6] years; P < .001); those aged 40 years and older had about 7 times the prevalence of disease as compared with those aged 24 years and younger (45.9% vs 6.6%; unadjusted PR, 6.95; 95% CI, 5.49-8.80) (Table 1).
Table Grahic Jump LocationTable 1. Prevalence of Coronary and/or Aortic Atherosclerosis by Demographic Characteristic

Lower education level and higher military entrance BMI were significantly associated with prevalent atherosclerosis, after adjusting for age. As compared with those who completed high school or less, those who completed at least some college had lower prevalence of disease (11.2% vs 13.8%; age-adjusted PR, 0.65; 95% CI, 0.45-0.92); this association did not extend to college or higher-level graduates. As compared with those with a normal BMI (18.5-24.9) on military entrance, those with a BMI in the overweight (25.0-29.9) or obese (≥30.0) range had a significantly higher prevalence of atherosclerosis (overweight: 12.7% vs 7.6%; age-adjusted PR, 1.39; 95% CI, 1.10-1.75; obese: 15.8% vs 7.6%; age-adjusted PR, 1.87; 95% CI, 1.35-2.60). Age-adjusted PRs by sex, race/ethnicity, occupation, service branch, active/reserve component, and military rank were not significant (Table 1).
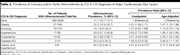
Age-adjusted atherosclerosis prevalence was associated with several diagnoses (Table 2). As compared with those with no major cardiovascular risk factor diagnoses, those with a diagnosis of dyslipidemia (50.0% vs 11.1%; age-adjusted PR, 2.09; 95% CI, 1.43-3.06), hypertension (43.6% vs 11.1%, age-adjusted PR, 1.88; 95% CI, 1.34-2.65), or obesity (22.3% vs 11.1%; age-adjusted PR, 1.47; 95% CI, 1.10-1.96) had a significantly higher prevalence of atherosclerosis. Of all risk factor combinations, only obesity and hypertension (n = 8) resulted in a statistically significant association after adjusting for age (50.0% vs 11.1%; age-adjusted OR, 3.14; 95% CI, 1.54-6.44).
Table Grahic Jump LocationTable 2. Prevalence of Coronary and/or Aortic Atherosclerosis by ICD-9-CM Diagnoses of Major Cardiovascular Risk Factors
Of the 464 service members with atherosclerosis at autopsy, only 2 (0.5%) had been clinically diagnosed with atherosclerosis and none had been diagnosed with ischemic heart disease.
COMMENT
ABSTRACT | METHODS | RESULTS | COMMENT | AUTHOR INFORMATION | REFERENCES
The prevalence of autopsy-determined coronary atherosclerosis among US service members was 8.5% in our study population. Older age; lower educational level; higher BMI at military entrance; and prior diagnoses of dyslipidemia, hypertension, and obesity were associated with a higher prevalence of atherosclerosis.
This prevalence demonstrates a steep decline from the rates of 77% noted in the Korean War5 and 45% in the Vietnam War7 (Table 3)—a decline that can be explained by either real or artifactual phenomena. Within the latter category are several methodological discrepancies among the 3 studies. First, while the Vietnam study employed angiography on perfusion-fixed coronary arteries, the Korean and current studies relied on macroscopic visualization, which is likely less sensitive to detect the earliest atherosclerotic changes. Second, the Korean study grouped fibrous thickening with fatty streaking as atherosclerosis, but it is now understood that intimal thickening may occur physiologically as a nonatherosclerotic adaptation.23 Third, while the Vietnam study used an absolute scale for grading plaque size, the present study enlisted the percentage-obstructed method used in the Korean study. Fourth, the autopsies in the earlier studies were conducted for scientific purposes, such as the study of wound ballistics, but the autopsies reviewed for this study were ordered to be conducted routinely rather than selected by specific patterns of injury; our method is therefore likely to have minimized expectation bias.24
Table Grahic Jump LocationTable 3. Coronary Autopsy Studies in the US Armed Forces: Korean War, Vietnam War, and OEF and OIF/OND

Selection biases may also attenuate direct comparisons of these studies. In light of the possibility that recent military volunteers have healthier cardiovascular profiles than their conscripted counterparts in the Korean and Vietnam wars, the potential emerges for a self-selection or “healthy warrior” bias when juxtaposing studies conducted during and after the draft era. In addition, advancements in battlefield medicine and technology may have saved the lives of wounded soldiers with atherosclerosis, who, by virtue of compromised perfusion, would have died in earlier conflicts; the prevalence of atherosclerosis at autopsy, in other words, may appear higher in the Korean and Vietnam wars because of unequal combat casualty care. Demographic and socioeconomic changes in the military population over this period may also account for the decline in atherosclerosis; because these data are unavailable for the Korean and Vietnam war studies, comparisons should be made cautiously. Finally, the smaller proportion of combat fatalities autopsied in the Korean and Vietnam war studies—less than 1% in both cases, as compared with more than 60% in the current study—may have resulted in less representative samples.
In light of historic epidemiology, these artifactual explanations are matched by compelling factual alternatives. Autopsies conducted for general aviation mishaps over the past 5 decades have generally demonstrated declines in any and severe coronary atherosclerosis, although shifting demographics complicate interpretation of these findings.25- 27 Less subjectively, prevalence of cardiovascular risk factors in the general US population,28- 32 with the exceptions of obesity33 and diabetes,34 are trending down. Although similar trend data are not available in the military, a recent study of more than 280 000 Air Force members found lower prevalences of hypertension, dyslipidemia, and diabetes as compared with the general US population.35 It is not unreasonable to assume that the prevalence of these risk factors among deployed US troops has declined since Korea and Vietnam. Smoking rates have also decreased in the military, often surpassing absolute rate reductions in the civilian population.31,36 The majority (51%) of service members smoked cigarettes in 1980, but by 1998 this figure had decreased to 30%.36 This 40% reduction in smoking prevalence within the military since the end of the Vietnam War likely contributed to our results.
Although the military culture tolerated or even promoted tobacco use in earlier eras, more recent Department of Defense (DoD) policy initiatives have aimed to reduce smoking. These have included discontinuation of cigarettes in K- and C-rations, efforts to deglamorize tobacco, and making Navy ships smoke-free.37 Current DoD Instructions seek to bring cigarette prices on military installations to within 5% of the local economy38 and to make DoD facilities smoke-free.39 Service-specific implementation of these policies have led to such initiatives as banning cigarettes from Air Force medical campuses40 and prohibiting smoking on submarines.41 Despite these policy initiatives and improvements, current military smoking rates (30.5%)36 continue to exceed civilian rates among similar age groups (21.4% in 18- to 24-year-olds and 23.7% in 25- to 44-year-olds).32
The findings of this study should be interpreted cautiously in light of its other limitations. Because autopsies were performed by multiple pathologists over the span of a decade, interobserver and intersession variation may exist. Studies by the World Health Organization, however, have demonstrated high reproducibility of coronary and aortic atherosclerotic grading among medical examiners and over time.42- 43 Based on the 2008 DoD health-related behavior survey, we also suspect that ICD-9-CM diagnoses failed to capture many cardiovascular risk factor exposures. In this survey of more than 28 000 active duty personnel, 30.5% had smoked cigarettes in the previous 30 days and 12.6% were classified as obese based on BMI.36 The degree of undercapture of these and other cardiovascular risk factors would likely not vary by the presence or absence of atherosclerosis, however, resulting in a nondifferential misclassification that would bias our results toward the null.
Our findings suggest that the prevalence of atherosclerosis has declined among deployed US service members since the Korean and Vietnam wars, and the work of Ford and associates3- 4 indicates that the prevalence of ischemic heart disease in the general population of US adults has declined over a similar time period. However, targets for further improvement remain. The 2008 DoD health-related behavior survey identifies smoking, obesity, diet, and physical activity as prime targets for public health intervention within the military community,36 and data from the National Health and Nutrition Examination Survey indicate that only 1.2% of US adults44 achieve the 7 lifestyle metrics15 correlated with a stepwise reduction in all-cause and cardiovascular mortality.44 To help “identify those personnel with a potential high risk for cardiovascular disease,”17 the DoD should consider automatic coding within their electronic health record for diagnoses such as obesity and smoking that are objectively measured during health care visits. Military and civilian health care systems should continue to help patients reduce their cardiovascular risk factors, beginning in childhood and continuing throughout adult life. Despite remarkable progress in prevention and treatment, cardiovascular disease remains the leading cause of death in the United States and other developed nations, and even small improvements in the prevalence of smoking and other risk factors may reduce death rates further and prolong healthy lives.45
